

Drug Policy Stuff This Week
Drug Policy Stuff This Week
DEA's position on weed, CDC overdose mortality figures show a slight decline, and Matthew Perry...

It’s been a pretty busy week in the world of drug news. After catching up on it all I thought I’d give readers a rundown of all the goings on.
Let’s start with what’s going on over at the good ole U.S. Drug Enforcement Administration. Yesterday, DEA published its formal proposal to reclassify marijuana as a less dangerous substance (schedule III). This marks the beginning of the public comment phase that will last for about 2 months. After just one day there are already over 563 comments posted. The comment period is sure to be heated and deeply polarized.
The first comment I clicked on at random simply said: “This rule is a horrible idea, this should remain in Schedule I. Marijuana is a gateway drug and ruins lives.”
The very next comment I clicked read: “I am shocked this is not fully legal. This plant has been subjected to so many lies for the republican party. I back full descheduling and full legalization.”
The DEA’s published proposal comes on the heels of an AP report exposing a rift in the federal government over marijuana’s reclassification. The White House, Department of Health and Human Services, and Department of Justice have seemingly all been on board with the rule change for many months while the DEA has remained a holdout. DEA’s top brass, Anne Milgram, refused to sign off on the reclassification. (This Milgram, who apparently refuses to bow to authority, is a case study that contradicts the findings of one Stanley Milgram).
It comes down to government agencies holding deeply divergent views. HHS said, “Although abuse of marijuana produces clear evidence of a risk to public health, that risk is relatively lower than…” the risk posed by many other drugs (in a lower schedule).
The DEA disagreed with HHS and Attorney General Merrick Garland.
In late January, according to AP, the DEA sent a memo to DOJ “seeking additional scientific input” on whether marijuana has an accepted medical use. This is the key question on which the whole regulatory overhaul hinges. Schedule I drugs are determined to be addictive and dangerous while not having any “accepted medical uses.” When it comes to marijuana, attorneys at the DOJ balked at the DEA’s “impermissibily narrow” criteria for determining medical use. I’m very curioius what those criteria were. (anyone who knows, shoot me an email).
I know that my Google Scholar search probably doesn’t meet the DEA’s standards. But out of nearly 1 million scientific articles generated in .1 seconds on the subject, surely there’s a few that spell out how marijuana is used medically.
After detailing the disagreement between federal officials, the AP pivots to a narrative of political intrusion. Just like drugs purport to hijack the brain, the DOJ “hijacked”the scheduling process:
“Several current and former DEA officials told the AP they believe politics may be at play, contending the Justice Department is moving forward with the marijuana reclassification because President Joe Biden wants to use the issue to woo voters in his re-election campaign and wasn’t willing to give the DEA time for more studies that likely would have dragged beyond Election Day.
Reading the political narrative I thought: So what? Of course drug scheduling is political. There is a long, long history of politics and racism and corporate interference determining US drug laws and their (ahem, selective) enforcement. Historians like David Courtwright and David Herzberg have chronicled centuries of “politics” influencing drug laws. The consensus among drug historians is that who is percieved to use a certain drug at a certain time tends to trump the objective properties of said drug.
Marijuana being legal in more than half US states and medical marijuana being legal even more leaves the DEA in an utterly bizzare political position. If they are keen on enforcing American drug laws, then how do they sleep at night with a Schedule I drug being sold at a store just blocks away from where I live?
I’m unsure of how this will end. But if the status quo doesn’t change, it will be yet another exhibit of a federal drug policy fossilized in the 1970s, causing all kinds of ridiculous problems. And, yet another example where President Biden looks aloof and impotent. If the President of the United States of America can’t muster the political power or capital to steamroll the DEA and Anne Milgram… yikes.
CDC Overdose Mortality: Deaths Decline
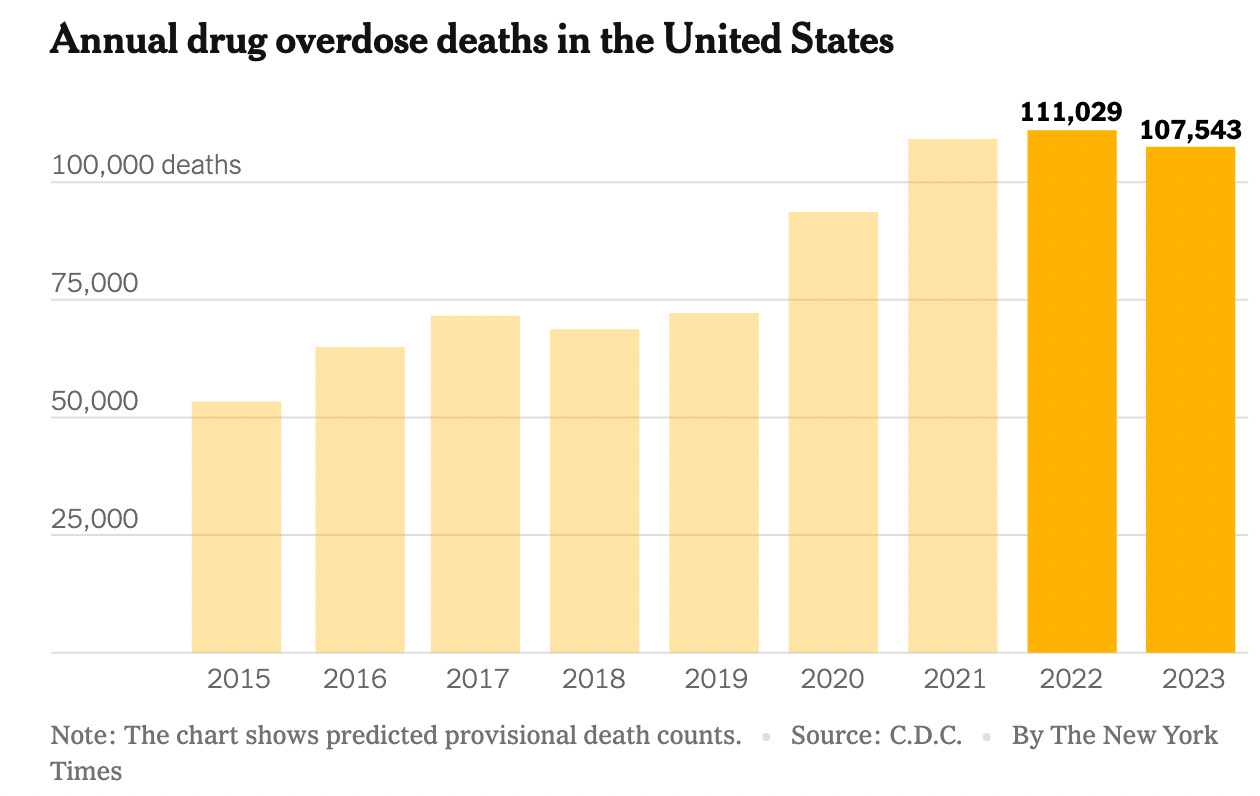
In 2022, there were 111,029 drug overdose deaths—the highest total ever recorded since the CDC started tracking overdose mortality decades ago. Last year, that number slightly declined to 107,543 deaths. A measly drop of 3,400 that could hardly be called a drop. It’s a tiny dip. And it leaves drug mortality at an absurdly high level.
There’s been some caveats and nuances in reporting these numbers. For starters, they’re most likely to be undercounting the true total. Many states record deaths differently. A number of cardiac events or cases of respiratory depression are overdoses but do not get recorded as such. The New York Times, for its part, asked whether Fentanyl has peaked? A sort of odd question to ask given this is just a small wobble after 100,000+ deaths for three years running. Not to mention, there is research that suggests deaths from drugs have been rising along an exponential curve for nearly five decades, since 1979. There’s been many wobbles off of that curve over the years, but drug deaths seem to constantly snap back.
(If you’re interested in that history then stay tuned for the next issue of The Baffler, where I criticize the idea that the US has suffered a decades-long string of bad luck with sucessive and overlapping drug epidemics. I just got my contributors copy and here’s a sneak peek).
More cautious reporting says now is no time to celebrate a small decline.
In 2018, there was a meager 4 percent decline in drug mortality. President Trump at the time took a victory lap. It was the first decrease in drug overdoses in nearly 25 years. Back then, people thought the 2018 dip could spell the beginning of the end. Finally, everyone thought, the trend is going down! Even if very slowly, at least its going in the right direction. But look what happened after that. Deaths spiked to unprecedented heights. Fentanyl headed west across the Mississippi, and deaths spiked in New Mexico, Arizona, Texas, California, and many others.
So what does 2023’s decline mean? It’s honestly too soon to say.
Fentanyl kinda has nowhere else to go. It has penetrated the entire market. This leads to a very grim takeaway: If the figures keep dropping from here, it may not be because policy prevented deaths, it may not be because our health care system started treating the sick, and it may not be due to a robust harm reduction safety net that kept people using alive. It might be due to the fact that everybody using is died. That has always been the grimmest end to this crisis. That synthetic drugs would simply rip through the population and this crisis won’t be stopped so much as burnt itself out, like the way a virus died because it killed all of its hosts before it could spread.
I hope that is not what happens. I hope it stops some other way.
Matthew Perry’s Death Investigation
When Matthew Perry was found dead in his hot tub, the medical examiner determined it was an accident. There was no foul play involved. Months later, the LAPD, with help from the DEA and the Postal Service, is looking into the source of Perry’s ketamine, and how Perry came to be in possession of it. This investigation implies that Perry’s ketamine was illicitly sourced from a dealer, and not prescribed for therapeutic reasons by a doctor. If it were the latter, it would be very easy to see who prescribed the drug.
Perry had previously said he underwent ketamine infusion therapy. Apparently, he had last been treated with the drug by a doctor more than seven days before his death. The medical examiner concluded that the ketamine he was on that day in his hot tub was probably not from a doctor. I think because of the high dose he was on? Unclear.
Either way, this sort of investigation tracks a clear pattern with law enforcement. From Prince to Philip Seymour Hoffman to “The Wire” star Michael Kenneth Williams, in all these cases where a famous person tragically overdoses, the police begin to look for who sold the drug, and then pursue a drug-induced homicide investigation.
It was especially ironic in Michael K. Williams’s case, where the actor starred in a show that deeply critiqued the American drug war and the police’s inept and futile role in denting the use and flow of drugs by disrupting drug dealers standing on a corner. It’s a show that exposes how the drug war corrupts all sides involved.
The police are looking at who distributed the ketamine to Perry. But what I don’t get is how they can pursue a drug-induced homicide charge given the circumstances of Perry’s death. It would be incredibly hard to argue in court that “but for” the ketamine, Perry would be alive. Not only does the whole drowning in a hot tub thing complicate that story, but Perry was on multiple other substances, in addition to having numerous serious pre-existing health conditions. Even healthy people are not supposed to be in a hot tub alone for more than 15 to 20 minutes. A very unhealthy person on ketamine and other substances being in a hot tub alone for who knows how long? Seems like a stretch to pin all of this on the ketamine. Should every dealer who sells ketamine be sure to tell their customers not to swim in any body of water alone?
At most, I can only see a distro charge for the ketamine. Trying to pin Perry’s deaths on whoever sold the substance seems like a huge leap. Guess we’ll see where this one goes.
That’s this week’s drug policy round up. Thanks for reading as always. And if you’re a paying subscriber, a big extra thanks.
Zach, thanks for your important important work, you're one of the few few voices of sanity and reality in this public health space!! I'm not the conspiracy theorist that this sounds like , but the DEA is the fascist-leaning enforcers of the drug war propaganda that NIDA has been empowered to spread. So, whoever heads the DEA will have a similar approach.
Good analysis Zach. Drug policy has always been political and always will be—since the Opium Wars perpetuated on China nearly 200 years ago—look where that’s brought us—China is playing the long game of revenge. Art of War.