

Few Mental Health Facilities Offer Medication for Opioid Addiction
Few Mental Health Facilities Offer Medication for Opioid Addiction
Despite high need, just one third of community mental health treatment facilities offer medications for opioid use, according to survey by RAND.

Only a third of outpatient community mental health treatment facilities (MHTFs) offer medications like buprenorphine, methadone, and naltrexone for treating opioid addiction, according to a new RAND study published in JAMA Network Open.
With the federal X-waiver requirement eliminated, with the Substance Abuse and Mental Health Services Administration guidelines encouraging all clinicians to screen for opioid use disorder and offer medications, with other incentives in place, lifesaving medications are still out of reach for too many people who need them.
The study, which surveyed a nationally representative sample, adds more texture and color to America’s treatment landscape, where gaps, silos, and missed opportunities abound. It’s as though addiction is supposed to be treated on an island somewhere far away. That attitude might explain why almost 90 percent of people with opioid use disorders do not recieve medication.
Increasing the delivery of medications in hospitals, emergency departments, primary care, and other “physical health” settings has been a major priority. There has been less focus on delivering these medications in mental health facilities. According to RAND, more than 13 million people have co-occurring mental health and opioid use disorders. If more mental health facilities screened and treated opioid addiction with the best medicine available, that could make a big difference in a lot of lives.
But that’s not what’s happening.
When it comes treating addiction, American health care appears to be stuck in the 20th century. After “detox” a person is shuffled through an intensive barrage of educational lectures, tons of group therapy, and pleasant enough recreational activities in bucolic settings (petting horses on a Malibu ranch). Meanwhile, they’re isolated from whatever environment in which their addiction flourished. Not a lot of people can drop out of their lives and go do that kind of treatment. It’s neither nor all that appealing. There needs to be way more options.
If you look at the number of people who need treatment but don’t want it, or the number of people who need treatment and want it but can’t get it, or the number of people who fatally overdose before they ever get proper care, if you look at all this and take it in, then you can see quite clearly that the dominant treatment model in America doesn’t work.
Why this study is important: Roughly 25 percent of adults with opioid addiction also having a co-occurring mental illness. That means mental health treatment centers serve as important touchpoints for dual-diagnosis treatment, where someone with, say, bipolar disorder, can also recieve treatment for an opioid use disorder at the same time and be treated by the same multidiscplinary care team. If only a third of community mental health treatment facilities offer medication treatment—178 out of 450 surveyed— then this isn’t what’s what’s happening.
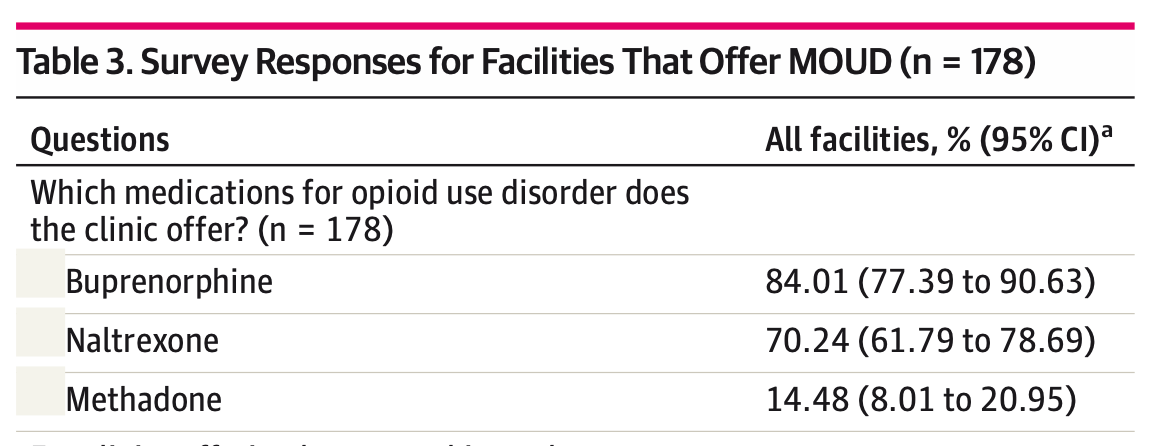
Of the facilities that do prescribe medication, buprenorphine was the most common, followed by naltrexone. Methadone (unsuprisingly) came in last, as it is stuck in the biggest silo of all. Only very heavily regulated clinics, of which there are too few, can prescribe methadone to people with opioid use disorders, and only under very strict conditions.
The most common form of payment for medication was Medicaid, which offers a glimpse into the patient population accessing mental health treatment with co-occurring substance use. This population tends to be adults who are poor, which speaks to the necessity of expanding Medicaid so more people can access quality treatment.
The Need for Integration
Substance use disorders fall under the broad umbrella of mental illness. And mental health treatment facilities are supposed to treat serious mental illnesses. According to the study, only half of treatment facilities reported screening patients for opioid addiction, while 20 percent reported not knowing the answer to the survey’s central question of whether medication for opioid addiction is offered.
This is a missed opportunity.
It speaks to the disjointed structure of health care in America, which places onerous burdens on prescribers and patients alike. In many of the “high need” states the RAND survey analyzed, reimbursement rates for addiction care is far too low. There is also a huge need for more health and social services on the patient side. Many have trouble getting on and staying on drugs like buprenorphine when so many other aspects of their life (housing, schooling, child-care, food insecurity, etc.) remains untenable.
Other states just makes it far too difficult to be on these medications. Some public and private insurers require approval before buprenorphine can even be prescribed. This delays access when time is of the essence and any delay can be costly. Other states require counseling as a condition for patients to receive methadone and buprenorphine, despite multiple studies showing that medication alone—without counseling—lowers overdose death rates and improves retention in treatment.
There’s also the strange idiosyncrasies of American addiction treatment. For many years, addiction treatment flourished outside the realm of traditional medicine (hospitals, emergency departments, primary care, family doctors, etc.). As the overdose crisis continued to spiral out of control, as the need for medication became more and more urgent, there has been a push to treat substance use like any other illness. Anyone, at anytime, should be able to schedule a primary care visit—seen in-person or online—and be able to see a doctor who understands opioid use and who can prescribe the right medications that stabilize someone. Once the patient is over that first obstacle, they can start their living their life again.
Sadly, this remains a total fantasy. There is still a long way to go before American addiction medicine works this way. This is possible for some, to be sure. But on the more severe end of the spectrum, people often need a lot more services that just aren’t there.
Still, these medications are relatively safe and quite effective. They reduce the number of emergency department visits, which reduces the burden and strain on an already strained system. Crucially, these medications have been shown over and over again to reduce the risk of fatal overdoses. That last bit is extremely important in today’s drug supply that serves up ultra-potent fentanyl analogues, often mixed with more dangerous depressants and tranquilizers. It’s baffling that the crisis of overdose deaths has gotten this bad, even as the best remedies available are barely being used to their full potential.